
In Tanzania, professionals in healthcare, social welfare, child protection, HIV services, counseling, education, and humanitarian aid are routinely exposed to emotionally demanding situations. Whether supporting survivors of gender-based violence (GBV), assisting orphans and vulnerable children (OVC), managing mental health crises, or responding to poverty and family distress, the cumulative emotional toll on service providers is significant yet often underrecognized.
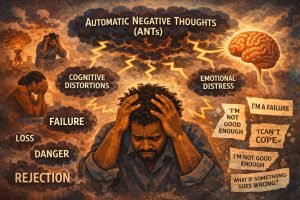
Frequently, the psychological impacts experienced by these professionals are simplistically categorized as “work-related stress.” However, a nuanced understanding distinguishes burnout, secondary traumatic stress, compassion fatigue, countertransference, and vicarious trauma. Discerning these concepts is critical for organizations, supervisors, and frontline workers across Tanzania.
1. Burnout: Systemic Overload
Burnout arises primarily from chronic workplace strain, driven by factors such as excessive caseloads, staff shortages, limited resources, inadequate organizational support, extended work hours, and lack of recognition. In many Tanzanian health and social service settings, professionals contend with overwhelming expectations amid systemic constraints, leading to emotional exhaustion, depersonalization, and reduced sense of accomplishment. Importantly, burnout is not inherently trauma-related but rather a response to sustained institutional pressure.
2. Secondary Traumatic Stress (STS): Absorbing Others’ Trauma
STS occurs when practitioners develop trauma-related symptoms including intrusive thoughts, anxiety, sleep disturbances, and hypervigilance following indirect exposure to clients’ traumatic experiences. For example, counselors repeatedly hearing abuse narratives, community case workers managing severe child neglect, or nurses witnessing traumatic injuries may manifest STS. In Tanzania’s GBV, HIV, mental health, and child protection sectors, this phenomenon is prevalent yet seldom discussed openly.
3. Compassion Fatigue: The Cost of Caring
Compassion fatigue emerges gradually from the cumulative emotional drain of caregiving. Helping professionals may experience numbness, emotional disconnection, reduced empathy, hopelessness, and chronic fatigue. Unlike burnout, compassion fatigue is directly tied to the empathic engagement with suffering individuals. It is especially relevant for counselors, social workers, nurses, community case workers (CCWs), psychologists, and caregivers in HIV and OVC programs.
4. Countertransference: Triggered Personal Narratives
Countertransference refers to the activation of a provider’s own unresolved emotions, experiences, or conflicts during client interactions. For instance, a counselor with a history of grief may become overwhelmed by bereavement cases; a GBV worker may react intensely to abuse disclosures due to personal history. Without clinical supervision and reflective practice, countertransference can impair professional judgment and service quality.
5. Vicarious Trauma: A Transformative Shift in Worldview
Vicarious trauma extends beyond exhaustion or distress. It denotes a lasting psychological transformation resulting from cumulative exposure to clients’ traumatic narratives. Over time, professionals may experience fundamental changes in beliefs about trust, safety, hope, relationships, spirituality, and meaning. A provider may come to view the world as inherently dangerous, lose emotional connection with others, or struggle with hopelessness about humanity. This is particularly pertinent in trauma-focused roles involving child protection, GBV response, mental health, crisis intervention, HIV/AIDS care, and humanitarian action.
Why These Distinctions Matter in Tanzania
Mislabeling these experiences leads to ineffective organizational responses. Common but inadequate approaches include addressing burnout solely with motivational talks, telling traumatized staff to “be strong,” promoting self-care while ignoring toxic workloads, dismissing the impact of repeated trauma exposure, and failing to provide clinical supervision or structured debriefing. Trauma-informed organizations recognize that safeguarding service providers is integral to quality client care.
Recommendations for Organizations
To strengthen workforce wellbeing, institutions should consider:
- Implementing regular supportive supervision and structured debriefing sessions
- Promoting workplace mental health awareness and reducing unrealistic caseloads
- Fostering peer support systems and offering confidential access to counseling
- Training leaders in trauma-informed management and psychologically safe environments
Concluding Reflection
Helping professionals are often expected to remain perpetually resilient. Yet sustained exposure to pain, trauma, and suffering exacts a profound psychological cost. As Tanzania continues to expand its health, mental health, HIV, education, and social welfare sectors, we must move beyond simplistic “stress management” rhetoric. Recognizing and mitigating the deep emotional and cognitive impacts of helping work is not optional it is essential.
Trauma-informed care must extend equally to clients and to those who serve them.